
I have been looking back at all of the work accomplished on health data exchange as well as some of the challenges that still remain.
In 2008, most of our healthcare system was still paper-based. Fewer than 10 percent of hospitals had implemented even a basic electronic health records system.
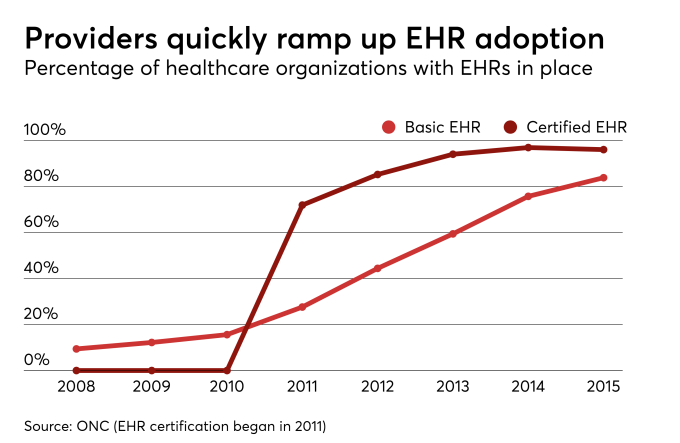
As we can see from the data, provided by the Office of the Nation Coordinator (ONC), a great deal of progress occurred from 2008 to 2015. Of course, much of this was a result of the federal incentives for EHR adoption incorporated in the Health Information Technology for Economic and Clinical Health (HITECH) Act. The HITECH Act was enacted as part of the American Recovery and Reinvestment Act of 2009, and signed into law on Feb. 17, 2009, to promote the adoption and meaningful use of health information technology.
HITECH provides financial incentives to “eligible professionals” and hospitals for the meaningful use of certified qualified electronic health records (EHRs). An eligible professional is generally a physician, although in the Medicaid program some mid-level providers were also included. CMS had major responsibility for the incentives (and penalties) hospitals and clinicians would receive broken into two separate programs, Medicare and Medicaid. With well over $ 30 billion in payments at stake, it is no wonder there was a sharp uptake in EHR adoption.
The ONC is responsible for the certification program for health information technology, which is required to be eligible for a payment or to avoid a penalty. As part of HITECH, the ONC also oversaw the $ 564 million State Health Information Exchange (HIE) Cooperative Agreement Program. In total, 56 states, eligible territories and qualified State Designated Entities (SDE) received awards.
This program was a big push towards interoperability and led to a rapid growth in the HIE market as well. As the work began to transition physicians and hospitals from paper-based to electronic systems it was critical for these systems to interoperate, allowing clinical data to flow between health care organizations.
Julia Adler-Milstein, from the Department of Health Management and Policy at the University of Michigan, along with David Bates and Ashish K. Jah, conducted a study published in Health Affairs in 2013. The results showed progress as the number of operational HIE organizations identified rose from 55 in 2009 to 119 in 2012. There were still some concerns however. Some technical challenges remained but primarily the issue was around a sound and sustainable business model.
As the authors stated, “Long-term financial sustainability for organizations facilitating health information exchange appears to be the most pressing challenge. The fact that three-quarters of efforts cite developing a sustainable business model as a major barrier is a warning to policy makers that the growth in health information exchange will likely falter unless these efforts become self-sustaining or there is a long-term public commitment to their financing.”
With no long-term commitment to public financing, and without a strong business model for sustainability on the horizon, many of these efforts began to falter at the end of the grant period. A 2016 study produced by NORC under contract with the ONC that only a small number of states were successful with significantly developing and implementing sustainable HIE systems.
At the time of the study, seven of the grantees were no longer in business and even fewer are in operation today. With the continued growth in digitization of health records in 2018 more than 95 percent of hospitals and nearly 90 percent of office-based physicians have implemented an EHR. So we started to see a picture where we had traded paper siloes of the past to the largely digital siloes leading into the present.
To address many of the concerns on building out a national infrastructure for health information exchange, in 2012 the ONC announced its plan for enforcing Conditions of Trusted Exchange (CTE) and Network Validated Entities (NVE). This approach was quickly discarded (although components are revived under the current ONC plans we will discuss later).
During this time a very successful open source effort overseen by the ONC called the Direct Project began. Launched as a part of what was then known as the Nationwide Health Information Network (NHIN), the Direct Project was created to specify a simple, secure, scalable, standards-based way for participants to send authenticated, encrypted health information directly to known, trusted recipients over the Internet. The Direct Project had more than 200 participants from over 60 different organizations, of which I was honored to be a participant.
After developing the standards and specifications for Direct, a series of pilots were initiated. One of which was the HIE in Oregon, which I had started in 2010, Gorge Health Connect, using a HRSA Planning Grant. Using Medicity iNexx software, we were able to quickly set up a Health Information Service Provider (HISP) to enable Direct secure messaging between provider organizations.
Very soon after the Direct Project initiatives started to scale across the country, a serious issue came to light—we need a security and trust framework that would enable participants to have some levels of assurance around identity and strong security. Thus was born DirectTrust, a non-profit organization created to solve for these issues and I was happy to serve as a founding member of the Board of Directors.
In March 2013, DirectTrust was awarded an ONC Cooperative Agreement to further work in accreditation, trust anchor distribution services, and governance of the DirectTrust community. The Cooperative Agreement was renewed for another year in 2014. Part of the Exemplar Health Information Exchange Governance Program, the grant was to “increase interoperability, decrease cost and complexity, and facilitate trust among participants using Direct for health information exchange of personal health information for health care improvements.”
Direct secure messaging was soon incorporated in standards and certification criteria by the ONC for use in the EHR Incentive Program. And the ease of integrating into a clinicians’ workflow made this a primary protocol for transitions of care. Those of us working on these efforts believed this could truly be a replacement for the fax machine in healthcare.
As David Kibbe, MD, chief executive officer of DirectTrust said in 2015, “In terms of new technology adoption, it’s been pretty fast, If you look at the growth of Direct over the past two years—and it’s only been three since it was available as a standard—it’s pretty astounding. We’re now up to 40,000 healthcare organizations that are contracted for Direct exchange by one of the HISPs in Direct Trust’s network.”
This year, the DirectTrust network saw 47.8 million health data exchange transactions in the first quarter, a 90 percent increase from the same time period in 2017. So we now have a way to push structured documents to known participants for clinical care.
But push is only half the story—what about querying for records? Remember the NHIN mentioned earlier—this was a cooperative established in 2004 under the ONC to improve the quality and efficiency of healthcare by establishing a mechanism for nationwide health information exchange. The group included federal agencies, local, regional and state-level Health Information Exchange organizations and private companies.
In 2012 the ONC transitioned the NHIN exchange to the eHealth Exchange. The participants who implemented the standards and services and executed the Data Use and Reciprocal Support Agreement (DURSA) legal agreement were now in the eHealth Exchange.
Overseeing the eHealth Exchange and defined in the DURSA is the Exchange Coordinating Committee. Shortly thereafter the Coordinating Committee designated Healtheway, a new nonprofit organization, to assume operational support of eHealth Exchange effective Oct. 1, 2012. The ONC said that the transition to a public/private partnership reflected their strategy to be an incubator for innovation and a focus on supporting a sustainable ecosystem of organizations that have found secure and scalable ways to exchange health information.
The eHealth Exchange has grown tremendously in the past decade. It is the largest and most successful health information exchange network in the country. The list of participants continues to grow and includes the Department of Defense, the Veterans Health Administration and the Social Security Administration. In 2015 Healtheway rebranded itself as The Sequoia Project.
Another important initiative overseen by The Sequoia Project is Carequality. Carequality was formed with an ambitious goal: to tie together the many valuable health information exchange activities occurring throughout the country, and solve the final mile of interoperability between them.
Another important effort began in 2013 named the CommonWell Health Alliance which went live in 2014. CommonWell, as it’s commonly known, is a nonprofit trade association, working to make interoperability an inherent part of health IT. Compose initially of some of the major EHR vendors it has grown in scope and importance over the last four years. CommonWell was inspired by former National Coordinator at the ONC Farzad Mostashari, MD, during a 2012 Bipartisan Policy Committee meeting where he challenged the assembled health IT leaders to come up with a market-driven solution to the patient identity problem since the government was unable to address the problem for them. Arien Malec and Dr. David McCallie who were serving on the Federal Advisory Committee to the ONC took up the call and CommonWell was eventually born.
Now things have changed considerably, with the passage of MACRA and the movement towards value-based care and payment models, and more recently the 21st Century Cures Act, which includes a number of interoperability provisions (including the TEFCA which I have written about here) there is a big policy push to improving interoperability. And the private market continues to innovate and technological solutions are flourishing.
Many of the standards and protocols for exchanging clinical information are developed by Health Level 7 or HL7. HL7 is a not-for-profit, ANSI-accredited standards developing organization dedicated to providing a comprehensive framework and related standards for the exchange, integration, sharing, and retrieval of electronic health information. And while messaging and structured documents are very important, healthcare has been slow to adopt modern web-based technologies used in other industries.
Then along came Graham Grieve and other thought leaders with the development of HL7 FHIR (for those wondering what that stands for it is Fast Healthcare Interoperability Resources). FHIR is a standard describing data formats and elements (known as resources) and an application programming interface (API) for exchanging electronic health records.
In 2011 Graham posted that HL7 needed a fresh look. The work began with a small team at HL7 developing the standard and after five years it has finally gained a good deal of traction. In fact Apple has partnered with a number of health systems to allow patients to access their health information right on their iPhone using the FHIR standards.
FHIR is designed specifically for the web and provides resources and foundations based on XML, JSON, HTTP, Atom and OAuth structures. Developers don’t need a great deal of healthcare experience to quickly being coding since these are the same standards commonly used across the Internet. And with the federal government strongly promoting the use of open application programming interfaces (APIs), FHIR is positioned to meet the needs of the healthcare industry and help take us into the future of interoperability.
And the other private sector initiatives are not standing still. The Sequoia Project (where I serve on the Board of Directors) recently underwent a significant reorganization to position itself for the future. CommonWell has become a Carequality Implementer and the eHealth Exchange has become a member of Carequality and is in the process of becoming an implementer.
“By reorganizing the eHealth Exchange and Carequality into separate legal entities, we further ensure unbiased, equitable treatment for the eHealth Exchange alongside every other implementer subject to Carequality oversight,” said Dave Cassel who heads up Carequality. With the eHealth Exchange and CommonWell now part of Carequality, and FHIR burning across the healthcare landscape, it seems despite the challenges ahead this past decade has shown significant progress in interoperability.

Brian Ahier
Brian Ahier serves on the Board of Directors for The Sequoia Project.