
HINGHAM, Mass. — “Is he going to make it?” Kim Bello asked, clutching her phone, alone in her yard.
She had slipped outside so her three children, playing games in the living room, could be shielded from a wrenching conversation with a doctor treating her husband, Jim. For two weeks, he had been battling the coronavirus at Massachusetts General Hospital, on a ventilator and, for the past nine days, connected to a last-resort artificial heart-lung machine as well.
The physician, Dr. Emmy Rubin, gently told Ms. Bello that while her husband had a chance of surviving, “If you’re asking for an honest opinion, it’s more likely than not that he won’t.”
Mr. Bello, 49, an athletic and healthy lawyer, had developed a 103 degree fever in early March after a hike in the White Mountains in New Hampshire and landed in a suburban emergency room six days later, struggling to breathe.
Now, despite all his doctors had done, his lungs looked white as bone on his latest X-ray, with virtually no air-filled spaces — “one of the worst chest X-rays I’ve ever seen,” Dr. Paul Currier, another of his doctors, said.
As he lay in the intensive care unit, even a touch that caused slight movement to his heavily sedated and chemically paralyzed body could send his oxygen levels into a tailspin. Doctors worried his heart would stop, and if it did, they realized they wouldn’t be able to resuscitate him.
They had tried everything to help him, including experimental drugs, a low-tech maneuver of flipping him on his belly to improve airflow and the most sophisticated life support machine.
They were considering one more “Hail Mary” medical maneuver, but setting it up required cutting the machine-supplied oxygen for 30 seconds, a gap they did not think he could survive.

“Even if those were things that could help him, trying to do those would kill him,” said Dr. Yuval Raz, a key specialist on Mr. Bello’s team.
Mr. Bello’s cataclysmic spiral from avid skier, cyclist and runner to grievously ill patient — and the heartbreaking and triumphant twists in doctors’ relentless efforts to save him — underscores the agonizing challenges confronting even highly trained physicians and well-equipped hospitals battling a ferociously capricious virus.
Hospitals have never before had, simultaneously, so many patients so sick that their lungs have basically stopped functioning. And while doctors are experienced at treating similar respiratory failure, the path of patients with Covid-19 can be maddeningly unpredictable.
“It’s like they fall off a cliff,” said Dr. Peggy Lai, a critical care doctor at Mass General. “You see young patients getting sicker and sicker by the day despite everything that you know is good standard of care.”
Without proven therapies to extinguish the infection, doctors ride roller-coasters of trial and error. They weigh risks of uncertain treatments and painstakingly adjust machines in hopes of shoring up patients’ lungs enough that their bodies clear the inflammation and heal.
“The tricky part with this disease,” Dr. Lai said, “is that we have nothing to follow, to know what predicts how sick someone will be and what predicts them getting better.”
On March 7, after Mr. Bello hiked Loon Mountain in New Hampshire, where his family has a condo and skis regularly, he was suddenly struck by a high fever.
After several feverish days, he developed a cough and chest tightness and visited a doctor, who prescribed antibiotics for pneumonia. But by March 13, he had so much trouble breathing that he went to a suburban Boston hospital’s emergency room. Doctors quickly decided he needed a ventilator.
“What if I don’t make it?” he asked his wife.
After she reassured him, she recalled, “He winked at me the same way he winked at me when we first met.”
Overnight, Mr. Bello was transferred to Mass General, becoming its first intubated coronavirus patient. His case initially seemed straightforward and manageable, said Dr. Currier, his first attending physician.
Like many Covid-19 patients, Mr. Bello had Acute Respiratory Distress Syndrome, or ARDS. His lungs were so inflamed and flooded with fluid that the tiny air sacs that transfer oxygen to the blood had become ineffectual sodden balloons.
Ventilator settings are precisely calibrated and continually adjusted: oxygen, breathing rate, breath volume and pressure. Doctors work to give enough pressure to keep airways open but not so much that lungs are overstretched and further injured.
Intubated patients are sedated and often given paralytic drugs so they don’t try to breathe themselves, allowing the machine to take over.
By the end of Mr. Bello’s first day at Mass General, the ventilator was supplying 65 percent oxygen, lower than what he’d needed upon arrival. The next day, it was further reduced to 35 percent, a good sign, given that the lowest setting, 21 percent, is equivalent to room air.
“He actually seemed to be improving,” said Dr. Currier, a pulmonary and critical care physician.
But then his condition inexplicably worsened, and his ventilator-supplied oxygen was ratcheted to the maximum, 100 percent.
Alarmed, around 2 a.m. on March 18, the medical team tried a maneuver called proning, Dr. Currier said. They carefully turned him onto his stomach to minimize the pressure of his heart against his lungs, decompressing his airways.
The results were encouraging. “This is great,” Dr. Currier thought before grabbing some sleep. “We fixed him.”
But as the day progressed, Mr. Bello’s blood oxygen levels plummeted.
Doctors had already started him on medications that many hospitals are trying: hydroxychloroquine, the anti-malarial drug President Trump has promoted; and a statin, which was eventually stopped because it affected his liver. He was also enrolled in a clinical trial of an antiviral drug being tested for Covid-19, Remdesivir, although nobody knew whether he was receiving it or a placebo.
That afternoon, increasingly concerned about his lung inflammation, doctors tried an immunosuppressive medication, tocilizumab.
Nothing was working. So doctors turned to an 11th-hour method. An eight-person team repositioned Mr. Bello onto his back, inserted large tubes into his neck and leg, and connected him to a specialized heart-lung bypass machine.
Called extracorporeal membrane oxygenation, or ECMO, the technique siphons blood out of the patient, runs it through an oxygenator and pumps it back into the body. It is intricately challenging to manage and isn’t available at many hospitals.
“ECMO is not a benign therapy,” said Dr. Raz, the medical director of Mass General’s ECMO department. “There’s a lot of bad things that can happen even with a good outcome.”
Risks can include bleeding complications and strokes. ECMO specialists must continually ensure that the blood volume circulating through the machine isn’t too low or too high, so that patients don’t get too much fluid and their blood vessels don’t collapse.
So far, ECMO has been used for hundreds of coronavirus patients worldwide, according to the nonprofit Extracorporeal Life Support Organization. Most are still on the machines, and data is incomplete, so survival rates are unclear.
“ECMO doesn’t fix anything,” Dr. Raz said. “It keeps you alive while other things, hopefully, take place.”
Mr. Bello’s lungs were so stiff that his “lung compliance” — a measure of elasticity that is usually over 100 in healthy people and about 30 in people with severe respiratory failure — was in the single digits.
His lungs could handle breaths only the size of a tablespoon, a tiny fraction of a normal-size breath. Blood began oozing from around the tubes, so blood thinners were stopped, Dr. Raz said.
Chest X-rays documented the decline. His first on March 13 showed significant fluid and inflammation, but “you could still see the lungs,” Dr. Raz said. On March 18, the X-ray was worse, but lung space was still visible. By March 20, “he had essentially what we call a whiteout.”
Daily, doctors and nurses updated Ms. Bello, 48, who took a leave from her part-time marketing job to help their children — Hadley, 13, and twins Riley and Taylor, 11 — cope with their father’s illness. Ms. Bello also raised thousands of dollars to provide the I.C.U. with meals from local restaurants, along with other needs.
She and Hadley developed mild symptoms like chest tightness, but doctors had considered it unnecessary to test them for the coronavirus.
Because visitors are largely prohibited in order to limit the virus’s spread, a nurse, Kerri Voelkel, put the family on speaker phone in Mr. Bello’s room several times daily.
“Hadley would have baked a cake, and she would joke ‘It didn’t come out so good, Dad, I’m going to try again,’” Ms. Voelkel recalled. “Taylor said, ‘I did my soccer drills out in the backyard.’ It’s heartbreaking to be the caregiver standing there and listen to these children talking to their father.”
As of March 27, Mr. Bello’s ninth day on ECMO, there was no improvement. When nurses tucked pillows under him or subtly shifted him to prevent bedsores, his oxygen levels would crater.
Dr. Rubin called Ms. Bello to explain the gravity of the situation. If Mr. Bello went into cardiac arrest, she said, doctors didn’t believe they could revive him. Ms. Bello agreed to a do-not-resuscitate order.
“Be honest,” she implored Dr. Rubin.
Dr. Rubin assured her they were not giving up and Mr. Bello could still survive. But, she said, “Honestly, I think all of our assessment at that point was that he’s probably more likely to die.”
Devastated, Ms. Bello rolled into a ball on the grass.
The following morning, March 28, the medical team dialed down Mr. Bello’s paralytic medication to see if he could manage with less, Ms. Voelkel said.
The effect was striking. “Jim woke up,” she said. He raised his eyebrows, and “you could tell he was trying to open his eyes.”
When prompted, he squeezed both of Ms. Voelkel’s hands. He nodded yes or no to simple questions. And when the nurses said they were going to adjust his position, he gave a thumbs up.
“We were like, ‘Oh my gosh, he’s in there!’” Ms. Voelkel said.
Ms. Voelkel described the scene to Ms. Bello over the phone. That afternoon, the family’s golden retriever, Bruno, grabbed Mr. Bello’s Boston Celtics cap, holding it in his mouth. Ms. Bello texted Dr. Rubin a photo of the dog with the cap and wrote, “Please do everything you can.”
Dr. Rubin’s eyes welled up. “I give you my word that we are doing everything we can,” she texted back.
But later, several hours after the paralytic medication was stopped, Mr. Bello, alone in the room while nurses monitored from outside, shifted his body slightly, movement that increased pressure on his blood vessels. This happens normally when we breathe, but he was too unstable to withstand it, Dr. Raz said. His oxygen levels nose-dived.
Both Ms. Voelkel and Tyler Texeira, a respiratory therapist, threw on their protective gear and rushed in. “We rescued him, we got him back,” Ms. Voelkel said.
“This is a man who, his lungs are so bad that we can’t have him awake,” she said they realized. “So we had to re-paralyze him in order to essentially keep him alive.”
Doctors’ last option involved trying to drain more fluid by adding another tube to the heart-lung machine, a maneuver that would require a brief stoppage of oxygen flow from the machine.
“He was so tenuous that we felt honestly 30 seconds off the ECMO circuit, he wouldn’t survive that,” said Dr. Rubin, a pulmonary and critical care physician.
After her shift ended, Ms. Voelkel said, “I cried the whole way home.” She thought of the phone calls from Mr. Bello’s children, similar in age to hers. “The despair I felt that we couldn’t save this man was beyond anything I could comprehend.”
Dr. Rubin called Ms. Bello and suggested that she visit her husband that night, something she’d been allowed to do only once before. The hospital hallways felt eerie. She donned protective gear and entered his room.
“I felt like, ‘Oh my God, if I keep talking to him, if I talk to him for hours, maybe he’ll stabilize, and maybe he’ll be OK,’” she said. “I was just telling him how much we need him, he has to fight this, he cannot leave us.”
She was told she’d have 15 minutes, but was given more than three hours.
“I’m squeezing your hand right now, I’m holding your arm, I’m laying on your arm, I’m touching your head,” she told her husband.
Within three days, an X-ray showed hope — some clearing in his left lung.
“Then, it just started improving, slowly,” Dr. Currier said. “And then it just got dramatically better.”
On April 4, Mr. Bello’s 17th day on ECMO, Todd Mover, a respiratory therapist, suggested he might be ready to come off the machine. The next day, Mr. Bello was disconnected from ECMO. He remained on a ventilator, but began handling reduced oxygen levels supplied by the ventilator, so doctors started easing paralytic medication and sedation.
Days later, in a milestone, physical therapists sat Mr. Bello on the edge of the bed. Ms. Voelkel FaceTimed Ms. Bello. She saw her husband kick his leg.
“I love you, blow me a kiss,” she cried. Mr. Bello, groggy from sedation, breathing tube in his mouth, moved his hand to blow his wife a kiss.
On April 11, nearly a month after her husband’s hospitalization, Ms. Bello sat at their dining room table for another FaceTime session. She had her daughters sit across the table, to spare them the sight of their father on the ventilator. They held an iPad so their brother, Riley, who was in New Hampshire, could also listen and talk.
“Hi Daddy, it’s Hadley and Taylor. We miss you so much. Riley’s also on FaceTime with us. We just want to say keep fighting, and you’re going to be OK. We love you so much.”
Mr. Bello, unable to speak because of the breathing tube, lifted his head, opened his eyes briefly and waved his hand slightly. “Love, love, love,” his wife said.
Doctors said they did not know why Mr. Bello survived. Their best guess is time. Although in some cases, people’s odds worsen the longer they’re on a ventilator, other patients recover after long intubations. The doctors don’t know if any of the medications worked.
Dr. Currier said he wouldn’t be surprised if Ms. Bello’s visit helped.
“She was in there for three hours by the bedside,” he said. “It was at its darkest at that point in time. You just can’t underestimate how much a difference something like that makes.”
On April 14, Mr. Bello was disconnected from the ventilator and began breathing on his own for the first time in 32 days.
This time, when she received a FaceTime call from the hospital, his wife gathered the children around. On the screen, he whispered the first words he’d been able to say to his family in a month: “I love you.”
As he was wheeled out of the I.C.U. to a regular floor, the medical staff, previously despondent about his case, lined the hospital hallway, erupting in applause. He waved.
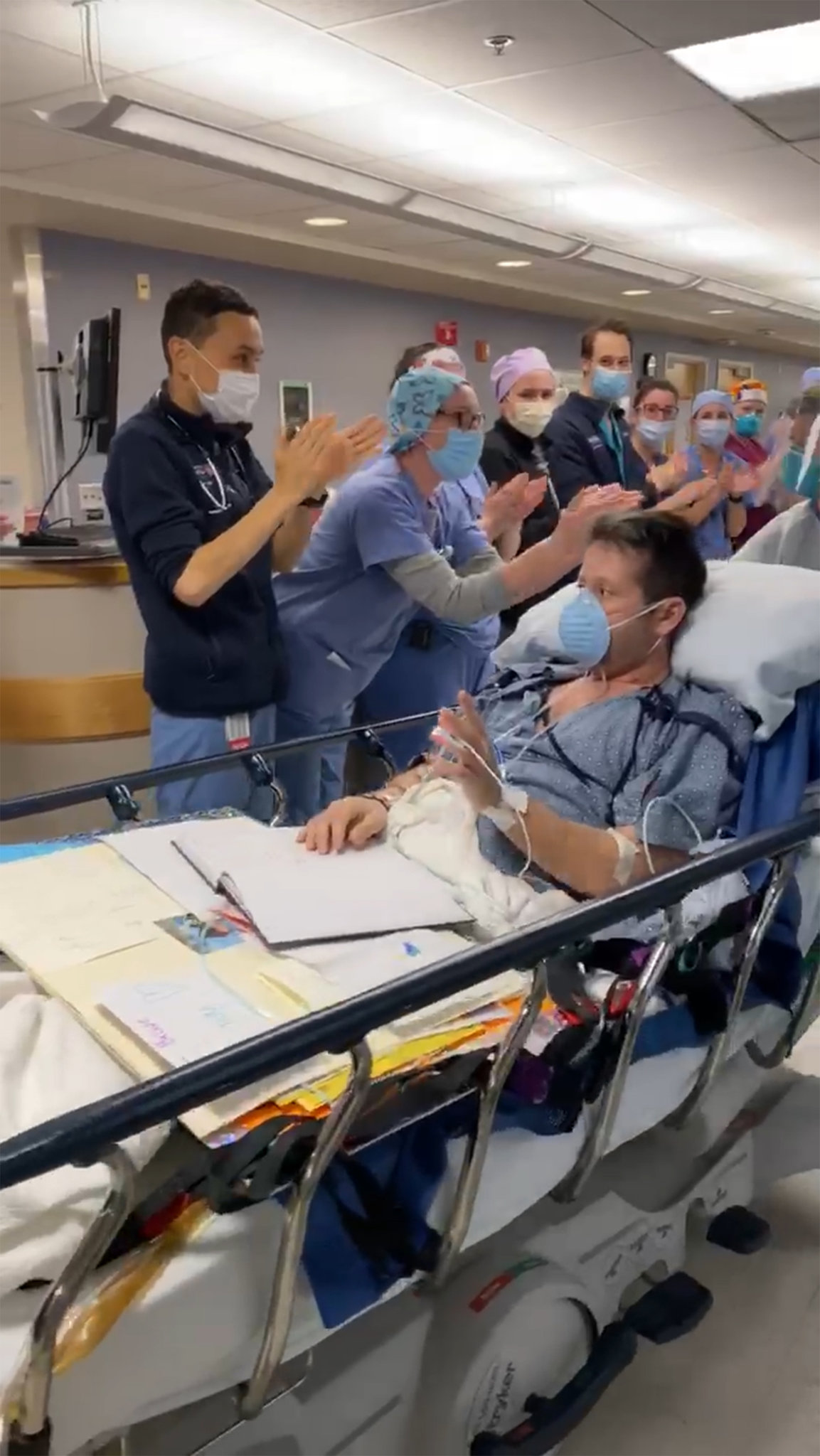
“It’s phenomenal,” Dr. Rubin said. Noting Mr. Bello’s previous health and fitness, she added, “everyone is very optimistic that he’ll have a full recovery.”
In brief comments from a rehabilitation hospital where he was transferred three days after coming off the ventilator, Mr. Bello said he was looking forward to getting back to working as a lawyer representing medical providers. “I’m alive today because of those very same people,” he said.
Already able to eat and to walk, he said he was proud of his wife and was eager to be back with his family.
Not long after that, on Friday afternoon, Mr. Bello came home.